|
OPINION BY MICHAEL BETRUS The media, politicians, and healthcare leaders have one-upped each other on COVID-19 restrictions for a year. For example, the Wisconsin Department of Natural Resources wanted their employees to wear masks. At home. While on Zoom calls. Pennsylvania told their residents to wear masks at home. Dr. Theresa Tam, Canada’s top health official, told everyone to wear a mask while having sex with a new partner. Then it happened. We reached our peak. But like the COVID-19 waves, there were three peaks. The CDC gets credit for all of this. It’s disheartening to pick on the CDC because there are some brilliant doctors and scientists that do incredible work. Still, it’s clear that after COVID-19, the leadership needs a change. They jumped off the mountain of public healthcare twice and flew off in a wing suit, trying to achieve Zero-COVID-19. If you follow extreme sports, you know how dangerous that can be. Just look up climbing great Dean Potter.  I watched Happy Days as a little kid. Even before the expression “jumping the shark” became a commonplace term, seeing Fonzie in real time, jumping a shark on waterskies while wearing a leather jacket, was just too much. Businesses have created products that jumped the shark. Many television shows have jumped the shark. You’ve probably had a dinner party when someone made a comment so over the top that you had to look down to see if they were wearing waterskis. The CDC did it with two different directors. Dr. Robert Redfield was appointed director of the CDC in 2018, and the CDC was the first to proclaim that wearing masks was necessary to curb COVID-19 transmission in the spring of 2020. The Mask Vaccine On September 16, 2020, Dr. Redfield spoke to a Senate committee. While holding up a disposable surgical mask (below), he said this: “We have clear scientific evidence they work, I might even go so far as to say that this face mask is more guaranteed to protect me against COVID than when I take a COVID vaccine, because the immunogenicity may be 70 percent and if I don’t get an immune response, the vaccine’s not going to protect me; this face mask will. Masks are the most important, powerful public health tool we have.” He said that the pandemic would be brought under control if Americans embraced mask-wearing for six to twelve weeks (just two more weeks!). He specifically called out 18-to-25-year-olds, whom he said are responsible for continuing the outbreak in America. The picture doesn’t show it, but Redfield must be wearing waterskis under that table. There’s a lot to unpack here. First, some percent of the population has natural immunity–T-cell immunity. We don’t know how much, but with so many people infected and asymptomatic (most of the infections), it could be 20-50% of the population. Second, the only way out of any pandemic is population, or herd, immunity. When a high percentage of the population acquires natural or vaccinated immunity, there just aren’t enough people able to pass it on, and it fizzles out. Third, the world had very high mask-wearing compliance. If masks are better than a vaccine, why didn’t it work? Anywhere? We cannot find a state in the country with sustained suppression of cases, hospitalizations, and COVID-19 deaths following a mask mandate. In January 2021, some inventive middle-schoolers took some leftover mannequins from one of the retailers that went out of business because of the lockdowns. For their science project, they placed a surgical mask on a dummy head and a cloth mask over the surgical mask. Double masking. They declared it more effective than single masking (it probably was). Except it wasn’t some middle-schoolers. It was the CDC:  The second shark jump: we need to wear two masks. On February 11, 2021, Dr. Fauci told Savannah Guthrie on TODAY that “two masks are better than one, it’s common sense.” First, this recommendation by the CDC came nearly one year after the initial face mask recommendation. We went from “mask science BC” (before COVID-19) that symptomatic individuals should maybe wear masks (a reasonable thought) to the CDC recommending everyone wear masks in March 2020, to this new recommendation of two face masks for everyone. How could a finding or recommendation like this take a full year? There was no real-world data that wearing two masks actually improved mask efficacy. In the mask-wearing universe, there are three segments of wearers: those that believe masks work and wear them with great discipline; those that wear them whenever they are required, the rule-followers; and those that rebel and either refuse to wear them or wear them as little as possible, adjusting their activities for a year to avoid wearing them. The middle group has lost confidence in the CDC and the effectiveness of masks to protect against COVID-19. The CDC should have identified by late summer 2020 that mask-wearing wasn’t stunting the spread: cases and hospitalizations in places with high mask usage weren’t any better than the places without mandates. A real study comparing people in two masks to those in a single mask, controlled by providing the masks for consistency, would have been valuable data. CDC Study on Mask Efficacy On November 27, 2020, the CDC released a mask study called “Trends in County-Level COVID-19 Incidence in Counties With and Without a Mask Mandate — Kansas, June 1–August 23, 2020.” The governor of Kansas issued an executive order requiring wearing masks in public spaces, effective July 3, 2020, which was subject to county authority to opt out. “After July 3, COVID-19 incidence decreased in 24 counties with mask mandates but continued to increase in 81 counties without mask mandates.”  The study was released in late November of 2020 but had a cutoff of late August. During the study period, COVID-19 hospitalizations in Kansas hovered around 300 a day against a capacity of 6,400, about 5% of capacity. In October, hospitalizations rose, like every state in their part of the country. By December, COVID-19 hospitalizations hovered around 1,000 a day for several weeks and then dropped sharply in January. Below is what happened with absolute numbers of cases during the CDC study period: 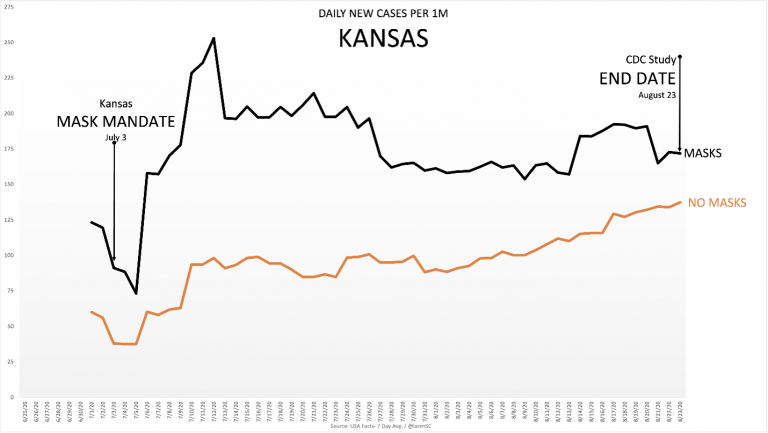 As you can see, the counties with mask mandates had more cases per capita during that period than those without mask mandates. Instead of comparing the case rate growth from July 3, 2020, when the mandate started, they chose to start by looking at the weekly case rate ending on July 9, after the masked counties had seen a huge increase. The seven-day average on July 3 was 91 per million. On July 9, it was 178 per million. They chose to start from 178. What that allowed them to do was claim a 6% decrease after the mask mandate, because they ignored the 96% growth in the first week after the mandate, giving themselves a higher baseline to start from. If you take the starting date of July 3 and the ending date of August 23, the case rate growth in the masked counties was 89%. If you start on July 9, it’s a 6% decrease. 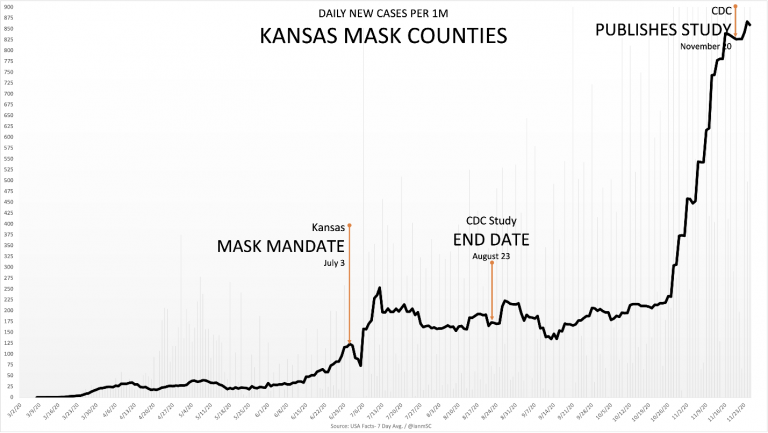 Further, you can see what happened to cases when the winter season hit the upper Midwest. The CDC cut off their study before the seasonal bump but released it well after cases rose. The CDC had this data but chose not to qualify their results, nor pull the entire study. Any time a study of this nature is completed and future data negates the conclusions, the study is supposed to be scrapped. In this case, it was released with no acknowledgement of what happened following the study period. From the time the study ended through the end of 2020, cases were about the same (actually lower) in the mask-mandated versus non-mandated counties. However, the burden is not on the non-masked counties to be better; having the same results nullifies the value that masks are supposed to bring to the table. The CDC had almost three months’ worth of data between the study’s end date and the release of the study. I went to my primary care physician in late fall 2020, and we discussed masks. He mentioned this Kansas study. I asked him if he knew what the data showed after the study cut-off date, and he did not. If there is one thing COVID-19 and the lockdowns should teach us, it’s that we should fact-check data ourselves before running with anything provided from just one source. CDC Study on Masks and Indoor DiningGovernor Greg Abbott sent shock waves through the country when he announced on March 2, 2021, that Texas would lift all restrictions and mask mandates a week later. Further, no city or county would be able to enact their own restrictions unless COVID-19 hospitalizations exceeded 15% capacity in that area. Texas is the second-largest and most powerful state in the U.S. behind California. It’s one thing when Iowa lifts all restrictions and quite another when Texas does. Nationally, the U.S. at the time had about 5% of total hospital beds occupied with COVID-19 patients (it’s likely that about 2/3 of them had a primary diagnosis of COVID-19). At what number do you go back to normal? New York City was under 1% when they would not send kids back to school in the fall of 2020. Texas lifting restrictions was the biggest step forward of the pandemic. When Mississippi followed suit (to some extent), President Biden called the decision by Texas and a Mississippi governors “Neanderthal thinking.” If Texas remains on its current trend of COVID-19 activity without masks and closures, how will other states justify the measures? You can picture Governor Newsom or Cuomo calling the White House in a panic. You can then picture someone from the White House calling the CDC in a panic: “Do something! You must put something out that shows this is a mistake, or they’re all going to open up by May 1!” Three days later, the CDC released this study: “Association of State-Issued Mask Mandates and Allowing On-Premises Restaurant Dining with County-Level COVID-19 Case and Death Growth Rates — United States, March 1–December 31, 2020.” Below are some key findings:
How much of an increase? Twice as much? Three to four times more? Ten times more? To write a paper and publish it, the authors would need to offer some very material differences in COVID-19 activity. They couldn’t jump the shark three times in six months, could they? If you play poker at all, you can relate to the expression that the CDC became “pot-committed.” They’d invested so much in the lockdown pot that they had to see it through. And so it went, with these startling conclusions from their ten-month study on mask-wearing and indoor dining:
The CDC is stating that not wearing masks and dining indoors caused about a one percent increase in cases and thus drew the conclusion that everyone should wear masks and not eat inside a restaurant. Any community college freshman stats student could tell you that one percent is within the margin of error and not statistically significant. The authors are further concluding that these NPIs contributed an additional 2.6% in COVID-19 deaths. It doesn’t pass the logic test. Half the deaths were to people at life expectancy with multiple underlying conditions. These are generally not people who are going out to dinner. You can argue that people in contact with them could have caught it and passed it on to those at risk. That is possible. This is where you encourage those individuals to practice more personal responsibility, not close hundreds of thousands of businesses indefinitely. America is pulling out of the pandemic and the lockdowns. The early CDC and WHO playbooks suggested a maximum of four-week closures for a Class Two pandemic like COVID-19. As we reach our one-year anniversary of the lockdowns, it’s time to get kids in class, get people back to work, and let everyone practice personal responsibility. Michael Betrus is the author of COVID-19: Lockdowns on Trial https://rationalground.com/the-cdc-jumps-the-shark/ References:
Comments are closed.
|
Archives
March 2021
|
||||||||||
 RSS Feed
RSS Feed